1 . INTRODUCTION
Fluoride concentration of groundwater in India varies noticeably. Drought conditions admit less water in aquifer system accelerates the fluoride ion dissolution from parent lithology. The presence of the accessory minerals, fluorite and apatite (Handa, 1975), cryolite and topaz (Madhavan and Subramanian, 2001) in the rock mineral assemblage are the major source for dissolution of fluoride in groundwater. In addition, minerals like biotite, muscovite and hornblende may contain considerable percent of fluoride (Madhavan and Subramanian, 2001). The weathering of host rock as the results of monsoonal water is the major phenomenon for existence of ionic fluoride in groundwater. Its concentration is restricted to its trace occurrence in basaltic aquifers. Lowering of water table during pre-monsoon period increases fluoride concentration in available water due to its high solubility. The consumption of fluoride through groundwater ingresses the human metabolism and chronic consumption leads to various health deformities like dental, skeleton fluorosis and nervous system impairment. In addition to this health hazard, renal system related illnesses are observed by some workers.
Averagely, 1 to 5% of world population facing urolith formation during their lifetime and is a most painful disorder of renal system (Sierakowski et al. 1979). Sudden increase in urolithasis episode in specific areas due to dominance in arid climate is exerting tremendous pressure on medical management of urolithiais. About 80% of uroliths are of calcium types (calcium oxalate monohydrate/di-hydrate, calcium phosphate and mixture of all in varied proportion), 10 to 15% of uric acid stone, 1 to 5% struvite stone and rare stone of cystein stone (Asper, 1984). The majority of reasons for urolith formation are dietary habits, dehydration, hereditary, life style, old age prostate disorder and powerful medicine used in diseases like cancers and AIDS (Costa-Bauza et al., 2007). However, increase in urolith patients in population suggest the role of environmental factors such as quality of water consumed as well as changing climatic conditions in urolith formation.
The renal system is responsible for excreting most of the body’s excess fluoride and is exposed to higher concentrations of fluoride than are other organs (Whitford, 1996). This suggests that it might be at higher risk of fluoride toxicity than most soft tissues. Muralidharan et al. (2002) studied the high fluoride concentration found in arid regions of Rajasthan state in India and the conclusion was drawn as causative minerals like calcite and dolomite have accelerated the leaching of fluoride to the groundwater. It is to be noted that from north India the relationship between fluoride concentration in drinking water and urolith prevalence in local population is reported by Singh et al. (2001). The review article by Ozsvath (2009) highlighted the relationship between fluoride consumption through groundwater and its effects on renal system. However, inadequate information is available on occurrence of urolithiasis (kidney stone disease) from basaltic areas where groundwater is amassed by fluoride concentration during drought situations and its health implications in the form of urolithiasis.
Increased urolithiasis episodes were observed in semi-arid Karha river basin, Maharashtra from Deccan Volcanic Province (DVP) of peninsular India during drought period and exact reason is quite obscure for medical professionals as the majority of urolithiasis in the area is neither having genetic origin nor anatomical reason. It necessitates understanding the possibility of environmental causative factors for urolith formation in the study area.
For this intend present study was undertaken to identify the urolithiasis occurrence with respect to consumption of highly mineralized groundwater.
2 . STUDY AREA
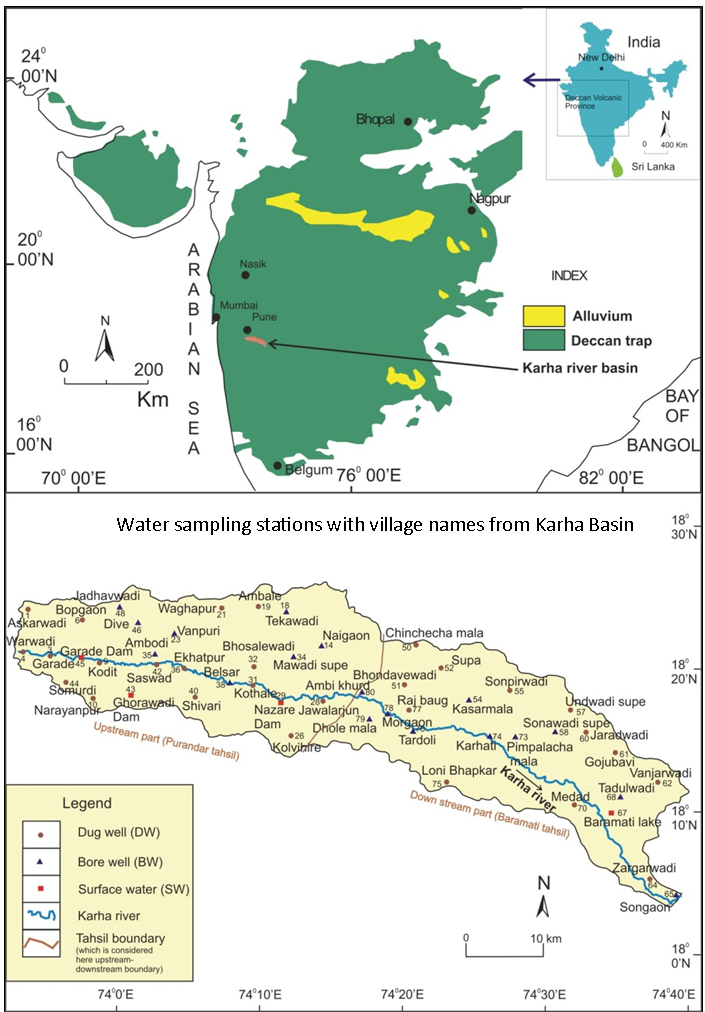
The area under investigation is Karha river basin (Figure 1) with a geographical area of about 1333 km2, from semiarid region of Deccan Volcanic Province (DVP). The Karha basin has geographical coordinates of 73º 52′ 07″ E to 74º 41′ 01″ E and 18º 3′ 41″ N to 18º 26′ 31″ N. The major settlements of study area are Saswad and Baramati.
Study area present in semiarid and rain fed region of Maharashtra. In year 2000 to 2004 drought situations were experienced due to declined annual rainfall < 550 mm. Such drought conditions developed the severe water scarcity in the region, which prompted people to depend upon highly saline water supply for drinking purpose.
Groundwater withdrawal is confined to vesicular, weathered, jointed and fractured upper basaltic crust, which is overlain by thin soil cover. Dug wells are the principal source of drinking water supply in the study area having average depth up to 10 m. Depleting groundwater levels are common in pre-monsoon season and condition being further aggravated by drought situations. Average groundwater level during pre-monsoon is 8 m whereas the water tables are fairly shallower during post-monsoon with an average depth of 4.6 m. The erratic nature of south-west monsoon is the controlling factor for groundwater chemistry variation.
3 . MATERIALS AND METHODS
To understand the temporal occurrence of urolithiasis from study area, previous 15 year data of hospitalized urolith patients was used. From this data, epidemic trends like number of urolith patients and gender class distribution were estimated. The information about number of 7081 urolith episodes reported in hospitals in the territory of study area (1994-2008) was procured for epidemiological study. Climatic data and groundwater quality data were acquired from government agencies namely IMD (India Meteorological Department) and GSDA (Groundwater Surveys and Development Authority), Pune, Government of Maharashtra. Number of summer hot days are calculated to their Tmax 97.5 > = percentile for 40.6ºC (Gadgil and Dhorade, 2005).
Further, spatial (village-wise) variation of groundwater fluoride data was used to correlate with village wise urolithiasis occurrence. For this purpose, 50 groundwater samples were collected from representative villages (Figure 1) during two consecutive post-monsoon (December, 2004) and pre-monsoon (May 2005) seasons. Physicochemical analyses of collected groundwater samples were carried out by using standard methods (A.P.H.A., 1995). In that, fluoride from groundwater was determined with SPADNS method by using Nano-colorimeter (500D) (Kale et al,, 2010).
The data was generated for average groundwater chemistry and urolith patient reported during respective years. Annual pattern of groundwater fluoride concentration and annual urolithiasis occurrence is correlated for temporal study. However, village wise occurrence of urolithiasis is used to correlate with respective groundwater fluoride concentration of dug well respective village.
4 . RESULTS
The results are shown in following two subheadings: 1) Epidemiology of urolithiasis 2) Intra-annual climatic variation and urolithiasis 3) Intra-annual variations in groundwater chemistry and urolithiasis, 4) Spatial distribution of urolithiasis and groundwater chemistry
4.1 Epidemiology of Urolithiasis
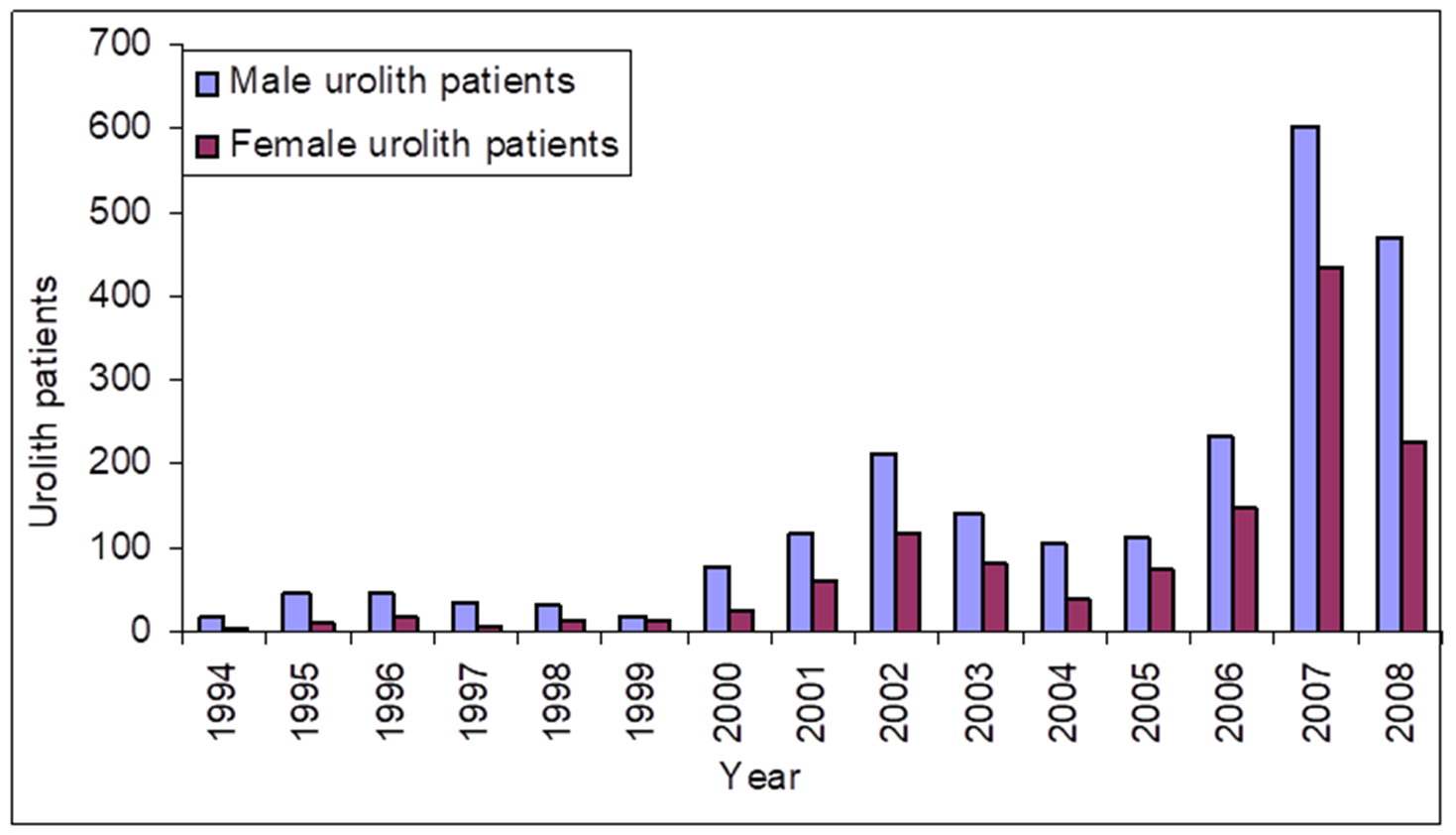
The urolith patient data of 7081 was procured from local hospitals and processed for its gender class as well as its annual distribution. Increasing trends of urolith patients are observed from year 2000 and male population is more prone to urolithiasis than female (Figure 2). The average male to female ratio of urolith patient is observed 2.88 (with SD 2.15) during period 1994 to 2008, indicating vulnerability of male patients for urolithiasis in the study area.
From medical records of hospitals more than 95% of uroliths are of calcium oxalate type and size ranges from 2 mm to 15 mm. However, few uroliths are bigger in sizes up to 75 mm in diameter are formed due to various anatomical disorders such as genetically originated, hyper calciuria generated, old age prostate
disorder and miscellaneous due to consumption of higher drugs in various treatments. Tiny uroliths of calcium oxalate are formed in majority of urolith patients from study area and altered geo-environmental and climatic conditions in drought situation are the focus points of present study.
4.2 Intra-annual Climatic Variation and Urolithiasis
Climatic data and urolith patient data of year 1994 to 2008 were used for temporal study (Table 1). More than 500 mm rainfall is observed from year 1995 to 1999 and substantial decrease (< 500 mm) is observed from year 2000 to 2003 (4 year). However, rainfall is increased from year 2004 to 2007. Total annual rainfall is poorly correlated to number of urolith patients reported in respective year. In less rainfall year of 2005, 2006 and 2007, number of hot days are showing more than 5 days and there is substantial increase in number of hot days 12 and 10 during year 2007 and 2008 respectively (Table 1). Number of hot days in a year is positively correlated (R2 = 0.8322) with urolith patients from study area. Generally, 1-3 hot days are experienced in study area per year but in drought conditions the number exceeds up to more than four.
Table 1. Annual weather station data corresponding to Karha basin
|
Year
|
Total annual rainfall in mm
|
Annual number of hot days
|
Total annual pan evaporation in mm
|
Total annual sunshine hours
|
|
1994
|
398.55
|
0
|
1960.7
|
2672.3
|
|
1995
|
731.05
|
1
|
1947.5
|
2758.1
|
|
1996
|
937.5
|
0
|
1981.9
|
2772.7
|
|
1997
|
376.5
|
0
|
1909.9
|
2907.3
|
|
1998
|
1046
|
3
|
1865.9
|
2684.9
|
|
1999
|
621.5
|
2
|
1720.5
|
2612.8
|
|
2000
|
342.7
|
2
|
1862.0
|
2841.8
|
|
2001
|
482.75
|
5
|
1756.4
|
2717.8
|
|
2002
|
238.9
|
8
|
1880.7
|
2791.0
|
|
2003
|
164.1
|
5
|
1843.5
|
2792.8
|
|
2004
|
567.5
|
1
|
1855.1
|
2811.2
|
|
2005
|
930
|
3
|
1754.9
|
2649.5
|
|
2006
|
971.5
|
4
|
1772.1
|
2616.6
|
|
2007
|
596.5
|
12
|
1858.4
|
2629.5
|
|
2008
|
470.5
|
10
|
1765.1
|
2579.7
|
a Rainfall is average values of Saswad and Baramati rain gauge stations,
bTemperature, pan evaporation and sunshine hours are of IMD Pune as a nearest weather station to Karha basin.
c Hot days are calculated at Tmax 97.5 > = percentile for 40.6
º C (
Kale et. al. 2014).
4.3 Intra-annual Variations in Groundwater Chemistry and Urolithiasis
Annual average groundwater chemical analysis data of 24 observatory wells of GSDA in study area was used to correlate with annually reported urolith patient (Table 2). Positive correlation (R2 = 0.7588) of average annual groundwater conductivity with annual reported urolith patients is observed from study area. Other groundwater ionic species such as Ca, Mg, Na, K, HCO3, Cl, SO4 and NO3 are showing meagre correlation with urolith episodes in the study area. Water types observed in year having rainfall > 500 mm is Ca+Mg-HCO3 and water type of Na+K-Cl+SO4 is dominated in year having rainfall < 500 mm. However, in the case of F ion there is significantly positive correlation with urolithiasis (R2 = 0.85).
Table 2. Annual averages of groundwater quality parameters from Karha basin during period 1994 – 2008
|
Year
|
W. L.
|
E.C.
|
Ca
|
Mg
|
Na
|
K
|
HCO3
|
Cl
|
SO4
|
NO3
|
F
|
|
1994
|
7.6
|
592.5
|
16.4
|
42.8
|
17.9
|
0.2
|
72.8
|
77.5
|
16.7
|
22.8
|
0.4
|
|
1995
|
7.5
|
676.9
|
54.1
|
38.6
|
22.1
|
0.2
|
124.6
|
170.0
|
47.0
|
13.4
|
1.1
|
|
1996
|
7.9
|
706.9
|
47.8
|
40.8
|
23.0
|
0.3
|
135.2
|
180.0
|
93.5
|
20.8
|
1.1
|
|
1997
|
7.5
|
745.0
|
25.3
|
25.9
|
22.8
|
0.4
|
130.0
|
115.0
|
37.7
|
23.0
|
0.5
|
|
1998
|
8.3
|
690.0
|
19.1
|
19.3
|
23.9
|
0.3
|
109.0
|
81.8
|
33.0
|
24.5
|
0.4
|
|
1999
|
8.1
|
687.5
|
22.8
|
22.9
|
28.9
|
0.7
|
101.5
|
84.3
|
31.0
|
26.0
|
0.5
|
|
2000
|
8.9
|
952.3
|
66.2
|
36.7
|
51.8
|
0.5
|
140.7
|
159.8
|
50.4
|
1.5
|
0.7
|
|
2001
|
11.1
|
1086.8
|
60.0
|
26.9
|
122.3
|
1.0
|
206.7
|
203.4
|
125.4
|
2.3
|
0.8
|
|
2002
|
12.0
|
1375.3
|
100.2
|
97.7
|
398.3
|
1.6
|
148.6
|
531.1
|
450.3
|
11.1
|
1.1
|
|
2003
|
17.0
|
1203.8
|
117.4
|
75.7
|
200.0
|
5.6
|
130.3
|
400.1
|
254.9
|
10.1
|
0.9
|
|
2004
|
18.0
|
999.7
|
104.0
|
50.2
|
173.7
|
6.4
|
99.5
|
272.5
|
94.0
|
3.2
|
0.8
|
|
2005
|
11.8
|
1112.2
|
55.8
|
29.9
|
103.2
|
6.6
|
162.0
|
158.9
|
96.6
|
16.8
|
1.3
|
|
2006
|
8.4
|
1797.3
|
44.1
|
58.8
|
202.8
|
7.8
|
328.0
|
226.0
|
131.8
|
18.8
|
1.5
|
|
2007
|
9.6
|
2015.9
|
76.3
|
60.2
|
323.0
|
5.2
|
202.0
|
284.7
|
349.4
|
26.1
|
2.9
|
|
2008
|
10.1
|
1283.0
|
56.6
|
42.8
|
231.8
|
3.9
|
170.0
|
217.5
|
219.0
|
20.6
|
2.3
|
a All parameters are in mg/L except W. L. is groundwater level in meters and electrical conductivity (E. C.) is measured in µS/cm. (
Kale et. al. 2014)
4.4 Spatial Distribution of Urolithiasis and Groundwater Chemistry
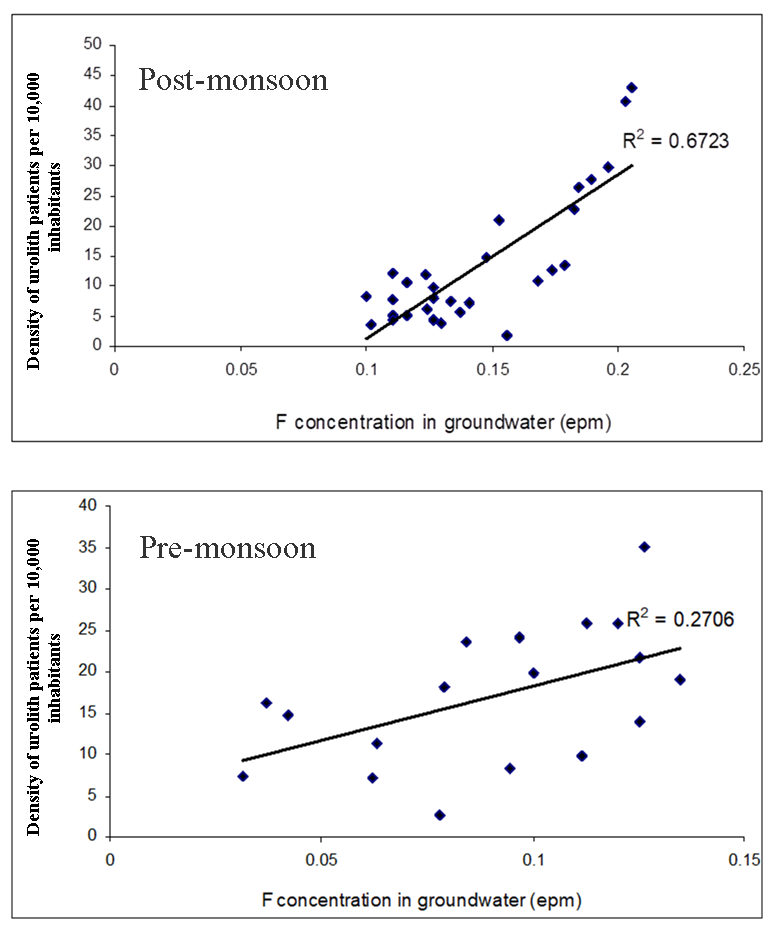
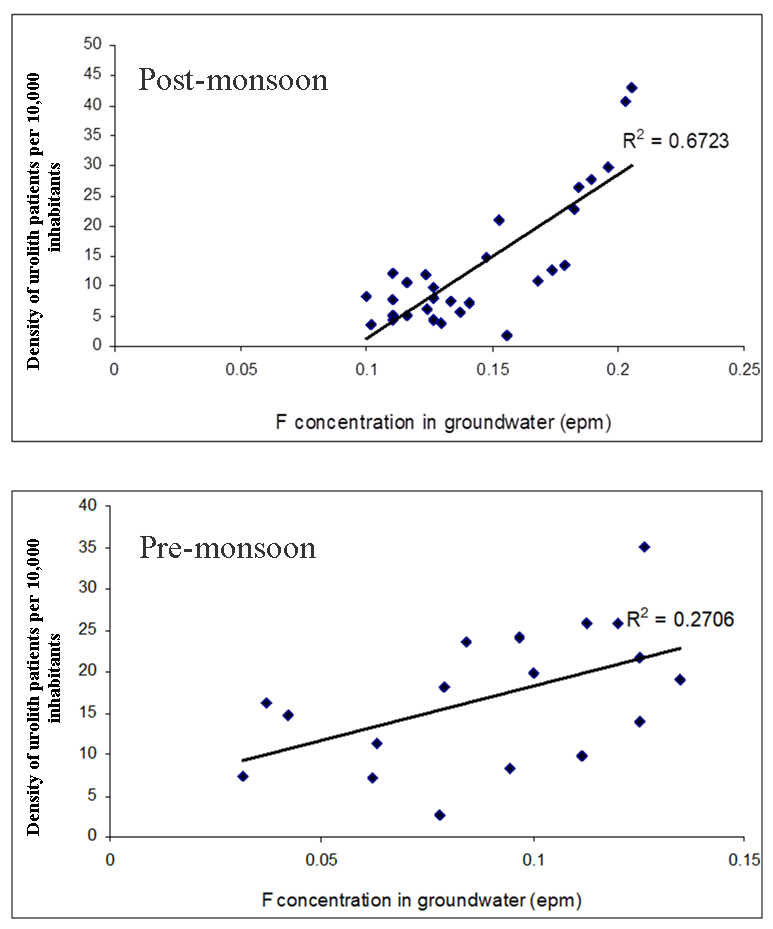
Spatial (village-wise) distributions of urolithiasis cases (during years: 2004 and 2005) and fluoride concentration in respective groundwater source was studied to understand their relationship. In post-monsoon (year 2004), urolithiasis occurrence was observed from 29 villages, however in pre-monsoon 18 villages are affected by urolithiasis. This urolithiasis occurrence were calculated for its density per 10,000 individuals (Indridason et al., 2006), however fluoride concentration is expressed in epm. In present study, maximum fluoride concentration observed in post-monsoon (December 2004) and pre-monsoon (May 2005) are 3.96 mg/L and 3.40 mg/L respectively. In post-monsoon season, village-wise density of urolith patients is convincingly correlated to groundwater fluoride concentration (Figure 3a). However, numbers of villages are decreased for urolith patient occurrence in pre-monsoon season and the positive correlation is observed with groundwater fluoride concentration (Figure 3b).
5 . DISCUSSION
5.1 Epidemiology of Urolithiasis
During year 1994 to 1999 urolith patients are observed less than 100 patients per year. This is due the satisfactorily rainfall experiences more than 500 mm, however consecutive decrease in rainfall (< 500 mm) for next four years showing continuous increase in urolith patients up to year 2008. As the groundwater is only source available for drinking purposes in the study area and people have to fulfil their drinking water need with depleted water source.
However, consecutive drought year increases mineralization potential of groundwater from study area due to decline in water level and evaporation dominance in semi-arid climate. This indicates that though rainfall is higher in post drought years the urolithiasis occurrence is increasing substantially. The groundwater mineralization potential is influenced by rainfall of previous year and groundwater exploitation.
5.2 Intra-annual Climatic Variation and Urolithiasis
In results of climatic variation and urolithiasis is shown in section 4.2, in that annual rainfall is poorly correlated with annual incidences of urolithiasis. Consecutive drought years depleted the groundwater up to its critical level and even if good rainfall years after drought also shows more groundwater mineralization potential. This situation is deprives the correlation between rainfall and urolithiasis. Consecutive drought years shows the cumulative built up of ionic concentration in groundwater from study are as the result of less water available for flushing of accumulated salts in vadose zone.
Further, number of hot days is convincingly correlated with urolithiasis in the study area. The reason for this is the heat stroke occurs that time the body is unable to regulate the temperature which causes rise in body temperature (Loughnan et al., 2010). Urinary tract stones in the regular season in summer heat caused are renal colic because of hot weather leading to substantial increase in human perspiration, resulting in severe loss of body water and reduce the urine volume (Chandrajith et al., 2006). Therefore, in the case of stone patients or potential patients with induced renal colic stone is the result of concentrated urine and allied compounds (Hassan et al., 2001) and finally results into urolith formation.
5.3 Basaltic Groundwater Quality Variation form Year 1994 to 2008
The water type of Ca+Mg-HCO3 dominance is observed during year during year which experiences rainfall > 500 mm. However, water type is shifted towards Na+K-Cl+SO4 during year experiencing rainfall < 500 mm as the results groundwater salinization due to depleting water table and evaporation dominance in vadose zone. The geochemical shifting of pristine alkaline aquifer condition to highly saline water dominated by Na+K-Cl+SO4 constituents.
In basaltic groundwater, ionic dissolution is predominantly derived from weathering phenomenon of ferromagnetic silicates (olivine and augite) and plagioclase feldspar. Also some ionic contribution is possible by dissolution of secondary minerals like zeolites. It is seen that fluoride concentration in groundwater correlates positively with urolith patient density (Figure 3: a and b), and finitely similar to work carried out by Singh et al. (2001), Pendse and Singh (1986), Kumar et al. (2003) in other geological setting.
The recent study in Yavatmal district dominated by basaltic lithology revealed that groundwater of the area is of bicarbonate (HCO3-) type and high fluoride (F–) concentration is observed in deeper aquifers compared to shallow aquifers (Madhnure et al., 2007). Pawar et al., (2008) reported the fluoride ingress in some dug wells exceeding the permissible limit (1 mg/L) of WHO from semi-arid DVP.
5.4 Fluoride Accumulation in Basaltic Groundwater in Drought Situation
Fluoride concentration increases in basaltic groundwater as the result of salinization during drought situation. This is due to the dissolution of secondary minerals in vadose zone. The fluoride concentration increasing above the 1 mg/L (WHO drinking water permissible limit) as the result of low amount rainfall (< 500 mm) is the alarming sign of provoking fluoride related illnesses. However, consecutive drought years (Section 4.2) shows the cumulative built up of fluoride in groundwater from study are as the result of less water available for flushing of accumulated salts in vadose zone.
It is interesting to note that fluoride is present in the urolith composition in the form of CaF2 (Kale et al., 2011). In north India the relationship between fluoride concentration in drinking water and urolith prevalence in local population is reported by Singh et al. (2001). The fluoride is most reactive anionic species it actively takes parts in many human physiological processes. At higher level concentration, sometimes it destroys the cell from various tissues from internal organs. This gives substantial pressure on renal system to filter out protein material of dead cell matter and possibly become nucleus in process of urolith formation (Rotily et al., 2000).
5.5 Role of Fluoride in the Formation of Uroliths
Some dental fluorosis cases are also observed in study area at the time of drought situations. However, no reports are available for skeleton fluorosis in study area. After integrating the entire results, the present study highlights the relationship between excess fluoride ingestion and urolith formation in the population from study area. Fluoride concentration in groundwater also directly affects nervous system in human beings (Alarcon-Herrera et al., 2001) and is linked with cell mortality rate in blood. This can allow higher oxalate generation due to process of dead cell protein breakdown, thus leading to nucleus for urolith (Alarcon-Herrera et al., 2001). However, more research is required from medical researchers in biochemistry point of view to understand the role of fluoride consumption to develop mass urolith epidemics. However, Susheela (1999) reported the other fluoride sources form diet ingredients may be one of the fluoride source.
Fluoride is essential for human in trace concentration to prevent dental caries, while exceeded concentration affects the teeth, bone and nervous system. The deposition of fluoride in the form of calcium fluoride was observed in the uroliths from Saswad (Kale et al., 2011). This indicates the role of fluoride in the formation as well as deposition in concentric layers of uroliths. Anasuya (1982) has demonstrated the relation between high fluoride intake and development of uroliths in rats. Vahlensieck (1985) has been noted the fluoride endemic area experiences the urolithiasis in Europe. However, Singh et al. (2001) suggested the proposed mechanism of fluoride participation of in the formation of uroliths. In his view, fluoride is indirectly increasing oxaluria by enhancing the absorption of oxalate from the intestine due to low availability of calcium.
There is no alternative of groundwater for drinking and cooking purpose for people residing in study area. In drought period, they have to be dependent on low yielding local aquifers. As fluoride concentration is increased due to cumulative accumulation triggered by insufficient rainfall, people are use this poor quality water directly for drinking purpose without physical or chemical treatment. As the result of this, consumption of fluoride rich groundwater has enhanced the urolithiasis in local population from year 2000 (Figure 3). This was evidenced by sudden increase of urolith patients as the drought strikes the study area (Figure 3). This necessitates the viable groundwater treatments before used as a drinking as well as cooking purposes to avoid such urolithiasis outbreaks.
5.6 Remedial Measures for Groundwater Fluoride Induced Urolithiasis
To avoid extra ionic load on metabolism water must be used with optimum mineral concentration (Sierakowski et al., 1979). The deionisers present in the market are found to be useful for this purpose. The use of surface sources for drinking e.g. river water or reservoir water need to undergo regular water disinfection with chlorination, Ultra-violet (UV) light treatment and reverse osmosis (RO). Especially, groundwater has to be filtered through reliable deionising unit before using it for drinking and cooking purposes. Groundwater from study area was contaminated due to considerable amount of fluoride that needs advanced treatments of defluoridation unit. The low cost treatments like using of alum and natural zeolites can be used for removing fluoride ions from groundwater. In low rainfall areas, rainwater is trapped with the help of roof top rainwater harvesting and the collected water can be used for drinking purposes with reliable treatments. With water treatment, study also warrants awareness of local people for drought condition and urolithiasis threats and further management of groundwater fluoride induced urolithiasis from semi-arid parts of DVP area.


 ,
N. J. Pawar 2
,
N. J. Pawar 2