Article Title :
Exploring Spatial Heterogeneity and Wealth-Driven Neighborhood Patterns in Health Insurance Coverage Among Scheduled Tribes in India 

9 (2025)
34-55
NFHS-5 , Marginalization , Insurance penetration , Indigenous health disparities , Geographical inequality , Spatial Analysis.



This study spatially analyzes localized geography of health insurance coverage among Scheduled Tribe (ST) households in India, revealing persistent regional disparities using nationally representative data from NFHS-5 and advanced spatial analytical techniques. Employing Exploratory Spatial Data Analysis (ESDA), Geographically Weighted (GW) correlation and Empirical Bayes Smoothing (EBS), the research identifies significant north-south and east-west rifts in economic status and insurance access. The findings reveal marked regional disparities, with significantly higher insurance coverage in southern and western districts, particularly in Kerala, Tamil Nadu, Andhra Pradesh, and parts of Gujarat compared to persistently low coverage in northern and eastern states such as Uttar Pradesh, Bihar, Jharkhand, and West Bengal. A Lorenz curve (Gini coefficient: 0.36) indicates moderate nationwide inequality in insurance coverage among ST households. Southern and western districts, notably in Kerala, Tamil Nadu, and Gujarat, exhibit stronger insurance penetration than northern and northeastern regions. While some ST populations in poorer northern areas benefit from targeted schemes, vast stretches of central and northeastern India remain underserved due to low economic development and weak healthcare infrastructure. Local Moran’s I analyses highlight High-High clusters in southern India and Low-Low clusters in the north-central belt, underscoring entrenched spatial disadvantage. The clustering effect suggests that health policy interventions in these regions have likely benefited from regional policy diffusion, where best practices and institutional capacities spill over into neighboring districts, creating reinforcing zones of success. Bivariate and GW correlation visualizations display a strong positive association between wealth status and insurance coverage, especially in southern and central regions. Conversely, regions with high proportions of BPL and poor ST households demonstrate strong negative correlations, indicating a double burden geography of economic vulnerability and exclusion from insurance schemes. Importantly, the findings emphasize the localized need for inclusive policy interventions to ensure universal access of insurance coverage for ST households, especially in identified vulnerable regions.
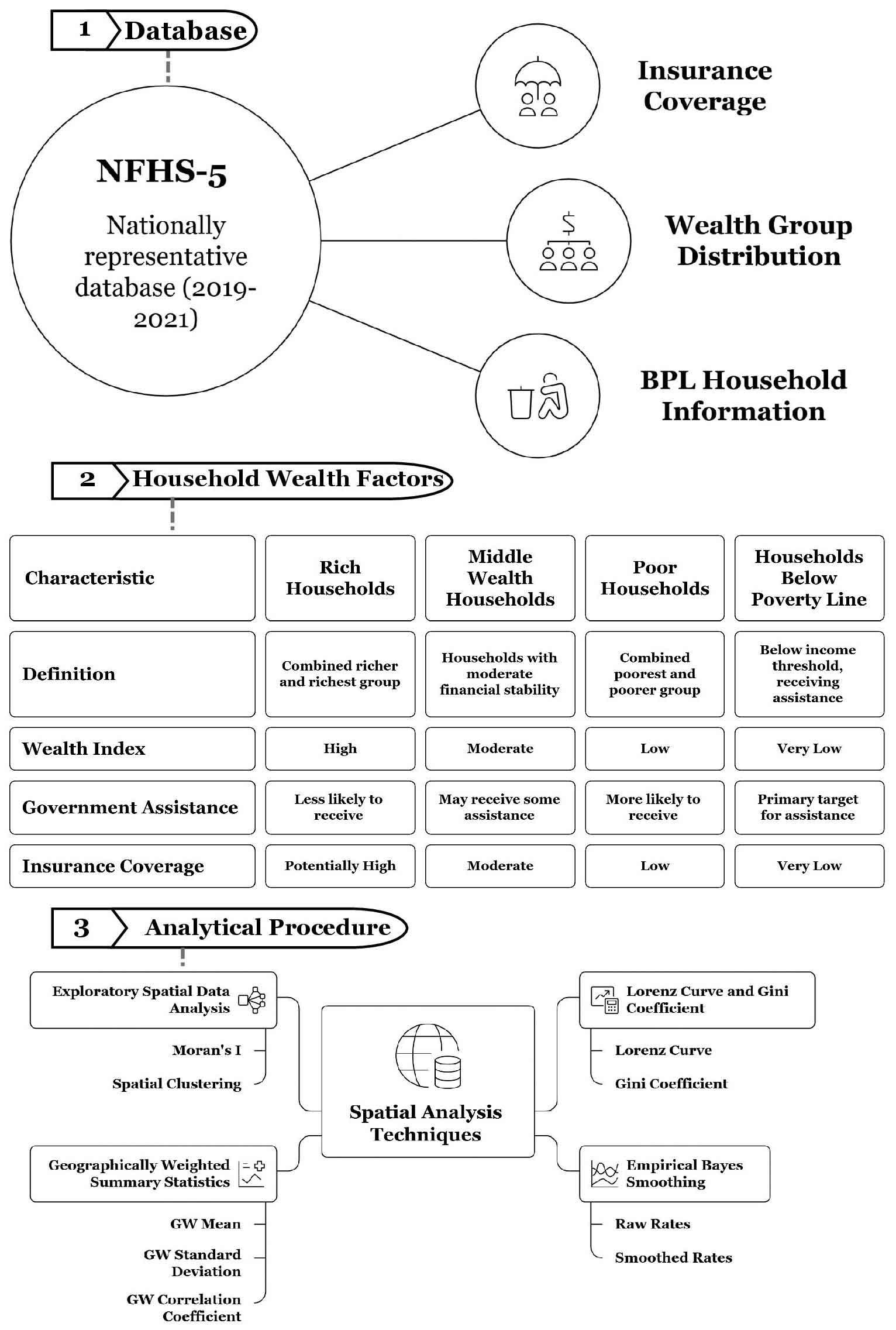
The study offers spatially explicit dynamics examining district-level heterogeneity of health insurance coverage among Scheduled Tribe households in India using NFHS-5 data.
A Gini coefficient indicates a moderate level of nationwide inequality in coverage among ST households, showing that the distribution is far from equitable.
Findings reveals significant north-south and east-west divides in health insurance coverage. Southern and western districts, including Kerala, Tamil Nadu, Andhra Pradesh, and parts of Gujarat, have significantly higher coverage, while northern and eastern states like Uttar Pradesh, Bihar, Jharkhand,
Identified “double burden geographies” where poor and BPL tribal households face both economic vulnerability and exclusion from insurance, with wealth positively linked to coverage in southern and central regions and strong negative correlations in poorer districts.
Revealed high–high coverage clusters in southern India, showing regional policy diffusion and positive spill overs.
Highlighted mismatches where wealth does not always translate into insurance. This persistent failure to address their unique cultural and environmental contexts has left healthcare as a
Bang, A., 2015. Health insurance, assurance, and empowerment in India. The Lancet, 386(10011), 2372-2373.
Planning Commission (Government of India), 2013. Twelfth five year plan (2012-2017): Faster, More Inclusive and Sustainable Growth. SAGE Publications India Pvt Ltd.
Player, J., 2025. Healthcare access in rural communities in India-Ballard Brief. Ballard Brief.
Rutstein, S. O. and Johnson, K., 2004. The DHS Wealth Index. DHS Comparative Reports No. 6. Calverton, Maryland: ORC Macro.
Rutstein, S. O., 2015. Steps to constructing the new DHS Wealth Index. Rockville, MD: ICF International, 542.
WHO [World Health Organization], 2025. Universal health coverage (UHC).